
Dermatofibroma
Author: Dr Amy Prideaux and Leo Sassoon
Chief Editor: Dr Daniel Keith
Dermatofibroma (DF) is a benign soft tissue tumour, composed of fibroblast and histiocyte proliferation. Clinical diagnosis of classical DF is usually straightforward; however multiple histopathological variants exist that can be harder to spot.
Macroscopic Appearance
As an aside, dermatofibromas may also be known as histiocytomas!
The macroscopic appearance of a dermatofibroma is usually a white or pigmented scar like spot with a surrounding rim of lighter pigmentation. They are a benign proliferation of fibroblasts and histiocytes of unknown cause. Some theories include preceding trauma such as an insect bite or aggressive hair removal. They are very common and most often occur on the limbs.

Macroscopic appearance in Fitzpatrick Skin Type 2

Macroscopic appearance in Fitzpatrick Skin Type 6

A further macroscopic example of a dermatofibroma on the foot of this patient with Fitzpatrick Skin Type 2 skin.
The Pinch Test
The pinch test can be used to make the diagnosis where pinching the skin causes a characteristic puckered appearance.



Macroscopic example of the pinch test seen here in a patient with Fitzpatrick Skin Type 5.
Dermoscopic Appearance

Under dermoscopy in this annotated example in Fitzpatrick Skin Type 2, the simplest appearances include:
-
A central white scar
-
Peripheral delicate network (you might think this looks like a group of small circles in the pigment)
These features combined with the pinch test would be very reassuring.

Unannotated example of the same lesion for comparison. This is a classical dermatofibroma!

Here is an annotated example in Fitzpatrick Skin Type 6.
As you can see the structure of the lesion is exactly the same as the example in Skin Type 2 above, with central scarring and a peripheral pigment network running around the entire central scar. The only difference here compared to the example in Fitzpatrick Skin Type 2 above, is the addition of more pigment throughout the lesion. The small circles making up the delicate peripheral pigment network can be very clearly visualised.

Unannotated example of the same lesion in Fitzpatrick SKin Type 6 for comparison.

Annotated example in Fitzpatrick Skin Type 5.
Features here show:
-
Peripheral pseudonetwork pigmentation blending into more dense homogenous central pigmentation
-
"Ring structure" - white lines surrounding central brown pigmentation (yellow arrow)
-
White globules (green circles)
-
White lines/network (red arrows)

Unannotated example in the same patient with Fitzpatrick Skin Type 5 for comparison.

Annotated example in Fitzpatrick Skin Type 5.
Features here show:
-
Dense central pigmentation with peripheral pseudonetwork
-
Partial ring like structure (yellow star)
-
White globules (green circles)
-
Comedo like openings (purple circles)

Unannotated example in the same patient with Fitzpatrick Skin Type 5 for comparison.
NB the ring shaped structures are a recently described sign unique to dermatofibroma in dark skin not previously included in text books.
A word of caution regarding Dermatofibromas!
What we have talked about so far is the most common appearance, however they can be quite polymorphic.


This schematic shows a summary of what dermatofibromas can look like.
Please do not feel you should reassure all patients with these features!
When you have a dermatofibroma which hits numbers 1-4 in the schematic and you are confident clinically that the lesion is a dermatofibroma, you can be reassured this is the diagnosis.
Below this, things become less specific and more uncertain. Therefore in the absence of other clinical examination findings, these should still be referred to secondary care.
Even in secondary care, these more atypical dermatofibromas may be excised for confirmation of the diagnosis, and to rule out amelanocytic melanoma.
Zaballos, Pedro et al. “Dermoscopy of dermatofibromas: a prospective morphological study of 412 cases.” Archives of dermatology vol. 144,1 (2008): 75-83. doi:10.1001/archdermatol.2007.8

Firm looking lesion on the arm, with some irregular white spots

Appearance under dermoscopy:
-
Central white scar like spots with surrounding vascular appearance
-
This is atypical and would not fit into the schematic 1-4. This example appears more like 7b.

Firm lentil like lesion on the forearm, but looks quite irregular.
Felt clinically like a dermatofibroma, and was in a typical location
The key message here is to refer if the positive features of a benign lesion don't add up, or if the lesion is too polymorphic. If you are unsure it's always better to refer so a biopsy can confirm the diagnosis.

Under dermoscopy you can see this looks quite different to the examples so far. You can see:
-
Central white scarred area with crystalline structures and a pale negative network
-
There is a delicate pigment network surrounding it but this is incomplete and irregular in pigmentation
-
It also appears unusually vascular
Therefore, this would be a complex/atypical mixed picture for a dermatofibroma.
This lesion was eventually excised due to the polymorphic and vascular nature of it. It's important to rule out amelanocytic melanoma in these cases where they can present with negative networks and polymorphic vasulature. The histology did however come back as a dermatofibroma!
Extension topic:
Aneurysmal dermatofibroma
As previously mentioned, clinical diagnosis of classical Dermatofibroma is usually straightforward; however multiple histopathological variants exist that can be harder to spot. This page extension will focus on one of these variants: Aneurysmal Dermatofibroma (ADF).
ADF can be challenging to identify due to its transitional morphology with another DF variant, haemosiderotic, which is thought to precede the development of ADF. Haemosiderotic/aneurysmal dermatofibromas (HADF) are rare but clinically important to recognise, as they can mimic melanomas and other non-melanocytic tumours, due to overlapping morphological features.
Macroscopic Appearance
Typical features:
-
Solitary, firm dermal nodules (sometimes papules/plaques)
-
Symmetrical shape and structure
-
Larger than classical DFs (>1cm diameter)
-
May have a haemorrhagic appearance
-
Most commonly found on lower limbs
Colour: HADFs are usually dark, ranging from bluish to purplish or dark-red.
The pinch test: HADFs, like other variants, generally show a positive dimple sign.
Below are some macroscopic examples of HADFs:

Macroscopic appearance in Fitzpatrick skin type 5

Macroscopic appearance in Fitzpatrick skin type 3

Macroscopic appearance in Fitzpatrick skin type 2
Dermoscopic Appearance
The most common features of HADFs are:
-
PHA = prominent homogeneous area (present in all lesions)
-
Involving at least 50% of lesion surface
-
-
PDN = peripheral delicate pigment network
-
SWS = shiny white structures
-
Includes shiny white blotches, strands and streaks
-
-
VS = presence of vascular structures
-
Red or pink visible blood vessels; often small dots in HADFs
-

Annotated example in Fitzpatrick skin type 5 featuring:
-
Prominent homogenous area
-
Peripheral delicate pigment network
-
Shiny white structures within the prominent homogenous area
-
No presence of vascular structures

Unannotated example of same lesion for comparison

Annotated example in Fitzpatrick skin type 3 featuring:
-
Prominent homogenous area (PHA)
-
Shiny white structures (SWS)
-
Vascular structures (VS)
-
No peripheral delicate pigment network
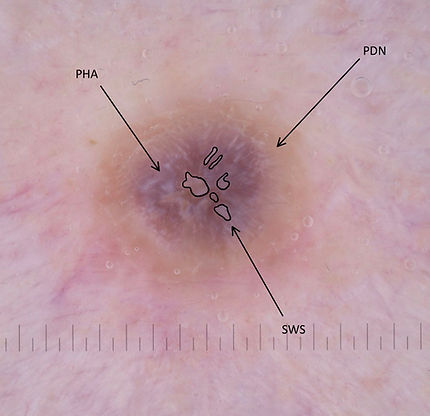
Annotated example in Fitzpatrick skin type 2 featuring:
-
Prominent homogenous area (PHA)
-
Peripheral delicate pigment network (PDN)
-
Shiny white structures (SWS)
-
No visible vascular structures

Unannotated example of same lesion for comparison

Unannotated example of same lesion for comparison
Symptoms
Often asymptomatic. However, patients may present with tenderness or pain and rapid lesional growth due to spontaneous intralesional haemorrhage.
Word of caution!
HADFs are highly polymorphic and are therefore considered an important differential diagnosis for more concerning lesions, particularly melanoma and other non-melanocytic tumours (e.g. haemangiomas, Kaposi’s sarcoma). In the absence of a peripheral delicate pigment network (PDN), HADFs become harder to identify due to the considerable dermoscopic overlap with melanoma.
Hence, when facing darker papulo-nodular lesions in which melanoma cannot be confidently excluded, the best option is to refer for excision and let histopathology confirm a diagnosis.